Positive vaccination messaging crucial for mothers

Dr Michael Gannon
Obstetrician & Gynaecologist at St John of God Subiaco Hospital.
Former President of the AMA (WA) and the Federal AMA
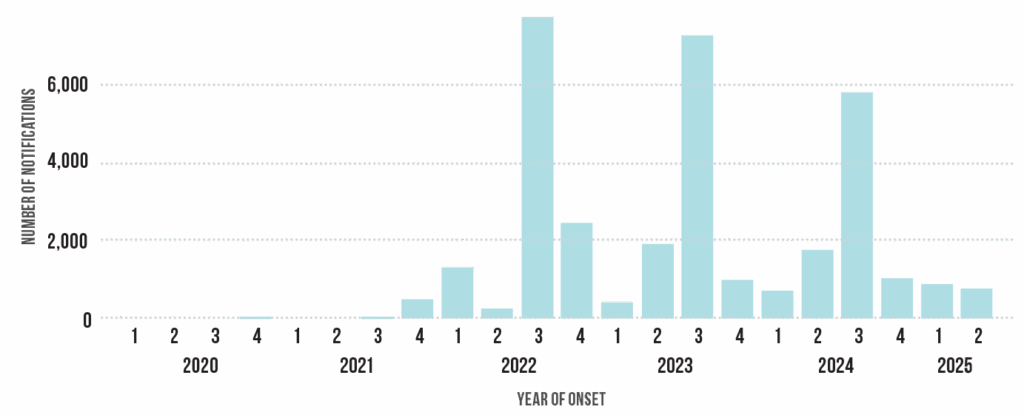
It has long been established that the most common reason for infants to present to their GP or an Emergency Department, to be admitted to hospital, or to be admitted in an Intensive Care Unit is bronchiolitis or pneumonia. Underlying this in a majority of cases is infection with Respiratory Syncytial Virus (RSV). By two years of age, nearly all children have been infected. The highly contagious virus typically causes symptoms similar to the common cold in immunocompetent adults. Earlier this year we saw the addition of maternal RSV vaccine to the National Immunisation Program (NIP).
 Mothers are invited to have the vaccination at 28-36 weeks of pregnancy, with subsequent production of antibodies crossing the placenta and passively immunising the fetus. This provides protection for the newborn for up to six months after the birth. While most reproductive-age women are unlikely to become ill themselves, it reduces the prospect of them passing on RSV infection to other vulnerable cohorts in the population, e.g. the grandparents.
Mothers are invited to have the vaccination at 28-36 weeks of pregnancy, with subsequent production of antibodies crossing the placenta and passively immunising the fetus. This provides protection for the newborn for up to six months after the birth. While most reproductive-age women are unlikely to become ill themselves, it reduces the prospect of them passing on RSV infection to other vulnerable cohorts in the population, e.g. the grandparents.
In my experience, the novel vaccine has proved acceptable to the vast majority of patients. There is no problem receiving the vaccine at the same time as Pertussis vaccination and/or Influenza vaccination.
Infants born to mothers who have inadvertently missed out on Abrysvo, or for any reason have a contraindication, can be vaccinated directly with Beyfortus (Nirsevimab).
These are exciting developments. Antenatal (passive) immunisation is acceptable to the vast majority of pregnant women. It has been consistently shown that positive messaging about the benefit or risk of vaccination from trusted antenatal care providers is an important part of the mothers’ decision making.
In my individual clinical practice, I have always strived to remove barriers to pregnant women receiving these vaccines. I see it as a very important part of the antenatal care I deliver to my patients. A patient who receives evidence-based advice on the safety of vaccination in pregnancy is not going to refuse the schedule of vaccines their newborn is offered under the NIP.
Do not forget this is a group of patients that collectively denies themselves perfectly safe things like caffeine, paracetamol and medium-rare red meat.